An anaesthetist will discuss the type of sedation used and the process they will follow with you. This procedure will not require a full general anaesthetic (GA). However, a local anaesthetic (LA) technique enhanced with intravenous pain relief and sedation will be employed where appropriate. You will be given the opportunity to ask any questions and raise any concerns you may have with your anaesthetist.
Once in the theatre suite, you will be connected to some monitoring equipment to measure your heart rate, blood pressure and the oxygen content of your blood. A needle or ‘drip’ will be placed in a vein, usually in the back of the hand. Then, you will be asked to lie face down on your tummy. Being in a comfortable position is very important when this procedure is done.
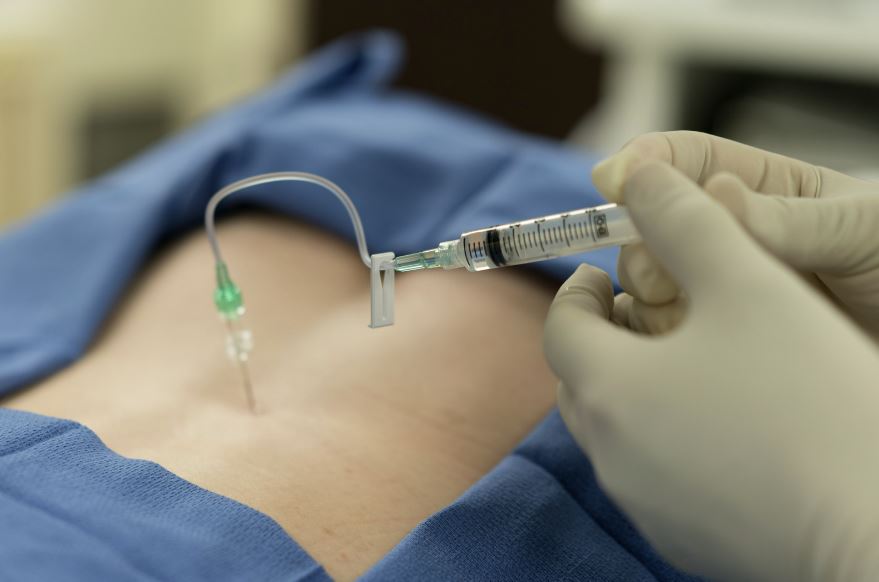
When this is achieved your back will be cleaned with an antiseptic solution, and some local anaesthetic will be introduced into the skin. When the skin has gone numb a needle will be introduced into the back very slowly and carefully. Once the needle is in the correct place in the epidural space, a single dose of medication will be injected and then the needle will be removed.
When the injections are completed, you will then be positioned in a way to make you as comfortable as possible.